autogenous reconstruction with inadequate soft tissue for either a second autogenous reconstruction or a Medpor reconstruction. In such a patient, a prosthesis may represent the only salvage procedure available.
Relative indications for the use of prosthetic reconstruction include a very low hairline where a temporoparietal flap would be required to allow autogenous reconstruction or extreme hypoplasia of the tissues with a concavity where the auricle will eventually be located.
Personal Thought on Surgical Reconstruction.The author has extensive experience with both the Brent and the Nagata techniques of auricular reconstruction and it is on the basis of that experience that the following comparative statements are made.
The Nagata procedure was designed to address the perceived weaknesses of the Tanzer/Brent technique, particularly the region of the concha, crus of the helix, tragus, and incisura intertragica. As such, the best possible Nagata-type result may have superior details to the best possible Brent-type result. The problem is that the “best possible results” do not occur most of the time.
The Nagata procedure, at least in the hands of this author, is definitely associated with a higher complication rate. The framework is of much higher profile, is much more complex in its details, and contains many more sutures. As such, the chance of cutaneous necrosis with framework exposure is significantly greater using the Nagata technique. On the other hand, these areas of exposure are generally small and heal without further surgical intervention and do not necessarily compromise the result.
The individual surgeon must decide, factoring in his/her experience, whether the possibility of a superior result is worth the increased risk of the Nagata procedure. In his own practice, this author currently uses the Nagata/Firmin technique in most patients. In patients with extremely tight skin, or the presence of other scars, the Brent technique is used because of its safety and reliability.
The other issue involves the chest donor site. The Nagata technique requires harvesting twice as much cartilage as the Brent technique. While Nagata harvests all cartilage subperichondrially, no detailed study has been performed comparing the chest wall deformity created by the Nagata technique at age 10 years with the deformity created by the Brent technique at age 6 years. Although the donor site is an issue not to be ignored, it tends not to be an issue regardless of which technique is used. Patients simply do not complain about the chest unless they are extremely thin.
Proponents of the composite alloplastic/autogenous reconstruction using Medpor cite the lack of chest donor-site scars/ deformity as an advantage. Although that is true, these same reports fail to mention the scars/deformity that replaces the chest deformity. For example, the composite technique robs the contralateral normal ear of all the skin behind it, resulting in obliteration of the sulcus or a skin graft donor-site scar if the retroauricular defect is replaced with partial-thickness skin. Additionally, this technique requires a scalp scar to harvest the temporoparietal flap. These scars are frequently hypertrophic and/or associated with thin strips of alopecia, which may be more troublesome to the patient than a chest wall scar.
Severe Facial Asymmetry
Placing the reconstructed ear in the best location is straight forward if the face is symmetrical or near symmetrical. In cases of significant asymmetry, however, compromises must be made. The surgeon cannot rely on measurements from landmarks such as the lateral canthus and oral commissure, because the entire side of the face is so much smaller than the other side. If such measurements were
chapter 27: ear reconstruction
used, the ear would be placed far too posteriorly and would appear strikingly abnormal. Of equal importance, however, the ear must not be placed too low or too anterior. The author attempts to place the ear in the correct craniocaudal position so that the earlobes are at the same level and then determines the anteroposterior positioning based on the relationship to the sideburn. No ear will look normal unless there is a sideburn in front of it.
Acquired Deformity versus Microtia
Total auricular reconstruction of the acquired deformity differs from congenital microtia. There is always less skin available. In microtia, removal of the cartilaginous remnant provides some supple, unscarred skin to supplement the retroauricular skin. In the acquired situation, there may be no residual ear skin, and the presence of scarring from the traumatic or surgical removal of the ear restricts the skin pocket. In many cases, a temporoparietal flap with skin graft is required in addition to the native skin. The flap provides an unlimited amount of vascularized tissue, but the combination of the flap and the skin graft never has the definition or color match of the native skin. In addition, the presence of an external auditory meatus limits the access incisions, the extent of the skin pocket, and the risk of infection. The canal is colonized with bacteria, frequently Pseudomonasspecies, which adds additional problems not encountered in microtia cases.
Special Situations
Acute Auricular Trauma and Cauliflower Ear
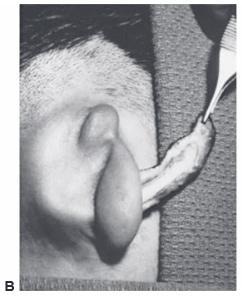
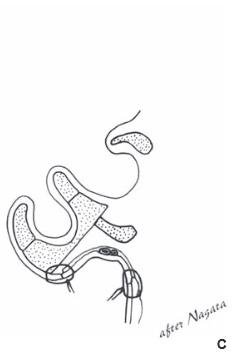
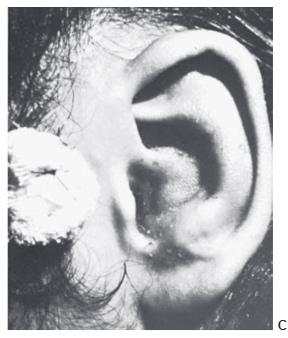
A hematoma may result from trauma and frequently occurs in wrestlers. Unless evacuated, the blood tends to become cartilaginous, resulting in the so-called cauliflower ear. Once fully developed, the cauliflower ear is extremely difficult to correct. Hematomas may require repeated aspirations or an incision to fully evacuate. Suturing gauze bolsters to the auricle to compress the skin against the cartilage usually prevents reoccurrence (Figure 27.18).
Amputated Ear
Most attempts to replace an amputated ear will fail, resulting in additional incisions/scars and “burning bridges” that may be useful for secondary reconstruction. The patient, however, will not easily accept the decision to discard the amputated part without an attempt at replacement. There is no easy answer.
Replantation of amputated ears has been reported and some excellent results have been obtained. The vessels are small, however, and failure is common. Any attempt at replantation must consider that success is unlikely and may result in scars that limit later reconstructive attempts. Incisions for the exposure of recipient vessels are kept to a minimum.
Reattaching large pieces of auricular tissue as composite grafts is doomed to failure. The good news is that such an attempt does not disrupt the surrounding tissues, does no harm, and makes the patient feel that “something” is being done.
Removing the skin from the cartilage and burying it beneath the retroauricular skin is a poor choice. The thin, delicate cartilage will not maintain its shape sufficiently against the forces of scar contracture. An alternative is to cover the de-skinned cartilage with a temporoparietal flap. The esthetic result will be poor for the reasons mentioned above and this useful tissue will not be available for secondary reconstruction.
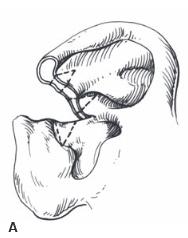
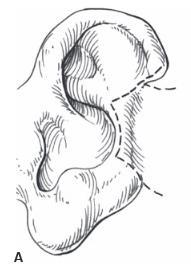
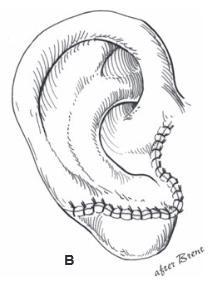
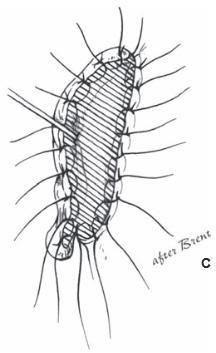
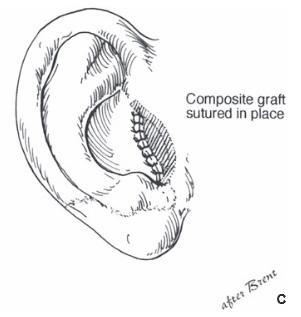
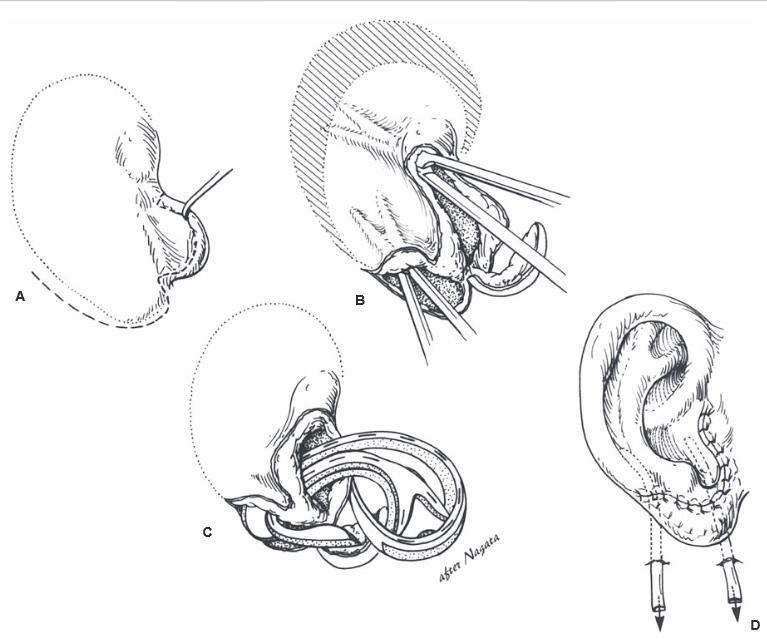
Several successful cases have been reported in which the posteromedial skin was removed from the amputated part, the cartilage was “fenestrated,” retroauricular skin was excised, and the part was placed on the healthy bed. The anterolateral auricular skin is vascularized through the